UDK: 616.613-007.43-073.756.8:004
Danailova M1, Chabukovska Radulovska J2,1 , Petrovska T2,1
1 Faculty of Medical Sciences, “Goce Delchev” University, Shtip
2 University Clinic for Surgical Disease “St. Naum Ohridski”, Skopje
Abstract
Trauma represents a significant public health problem with consequential socioeconomic costs. Isolated rupture of renal pelvis following a blunt trauma is a rare medical condition with very few case reports published in literature. We present a case of a male patient who was admitted to our hospital experiencing abdominal pain and not being able to urinate, prior having a fall from his own heigh few days before. After conducting multidetector computer tomography scan with contrast media of the abdomen, the leakage of the contrast media from the renal pelvic lesions in both kidneys was evident. The patient exhibited signs of recovery following the surgical placement of JJ stents in both kidneys which was evident on the control MDCT scan.
Key Words: blunt renal trauma, MDCT, renal pelvic lesions.
Introduction
Over the past two decades, there has been a constant improvement in the imaging and treatment of genitourinary trauma. The gold standard for the assessment of GU trauma today is multidetector computed tomography along with the use of intravenous contrast medium and the multiplanar reconstructions which provide fast assessment of the urinary tract, as well as coexisting intra-abdominal injuries. The necessity for imaging evaluation of the genitourinary system in medical practice fluctuates depending on few factors like the patient’s overall blood flow status, any accompanying injuries, the site of blunt or penetrating trauma and the presence of blood in the urine.Top of Form
Case Report
A 68-years-old male patient was brought to our Emergency Room complaining of abdominal pain, urinary retention and a history of falling from his own height four days before admission. To thoroughly assess his condition, after conducting a clinical examination and a blood test, it was recommended that an abdominal MDCT scan should be performed with two post contrast series, to provide a comprehensive evaluation.
Following the intravenous contrast injection, in the post contrast series, the kidneys exhibited appropriate absorption and excretion of contrast media within the expected time frame (in a timely manner). However, it was observed that the patient had extrarenal pelvis bilaterally, cortical cysts bilaterally that didn’t interfere with the urodynamic, dilated ureters along with a dilated urinary bladder. Furthermore, in the adjacent kidney tissue, there was observed leakage of the contrast media from the renal pelvic lesions in both kidneys. There were no indications of trauma to the parenchymal organs within the abdominal region.
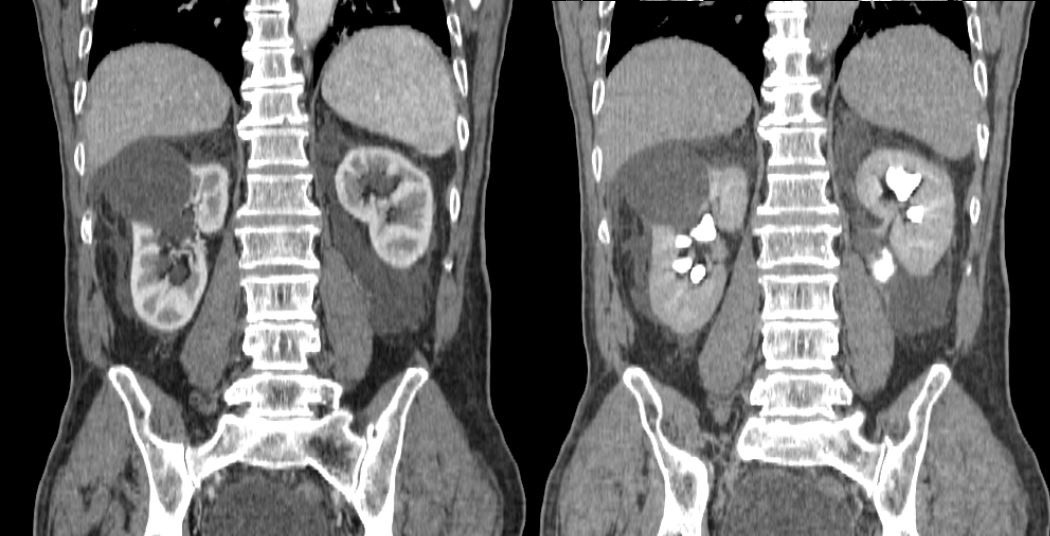
Figure 1. Free fluid in the surrounding kidney tissue.
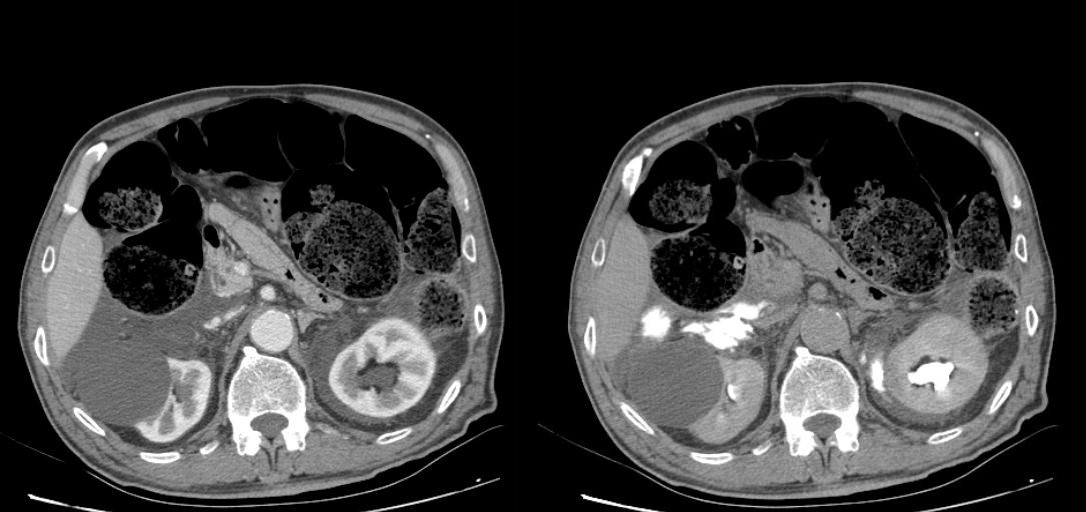
Figure 2.
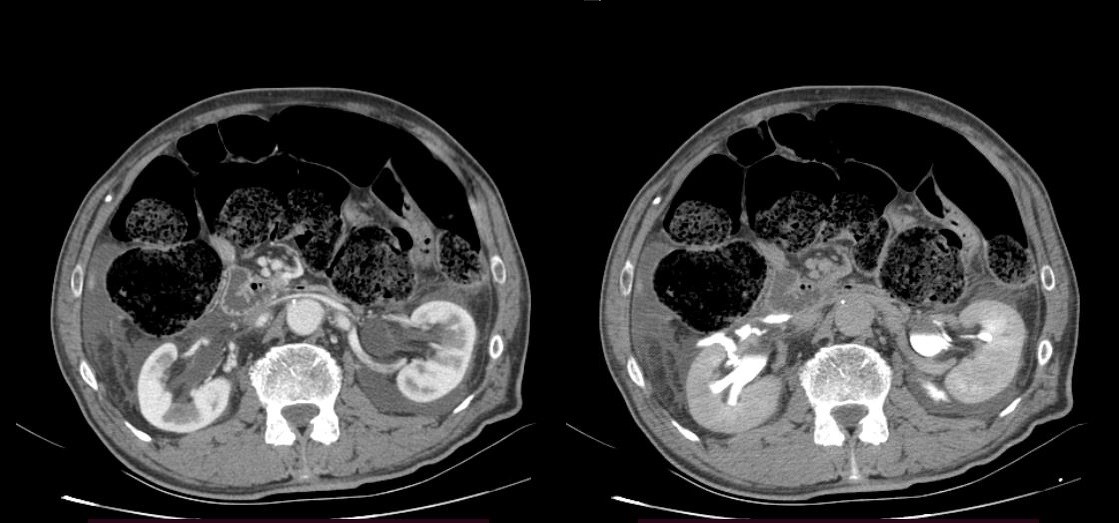
Figure 3.
Figure 2 and 3. As seen on the scans to the left, the surrounding free fluid dif. dx can mean urine, blood. On the scans to the right, the contrast media leakage is evident in the surrounding tissue, meaning there are lesions in the renal pelvis bilaterally.
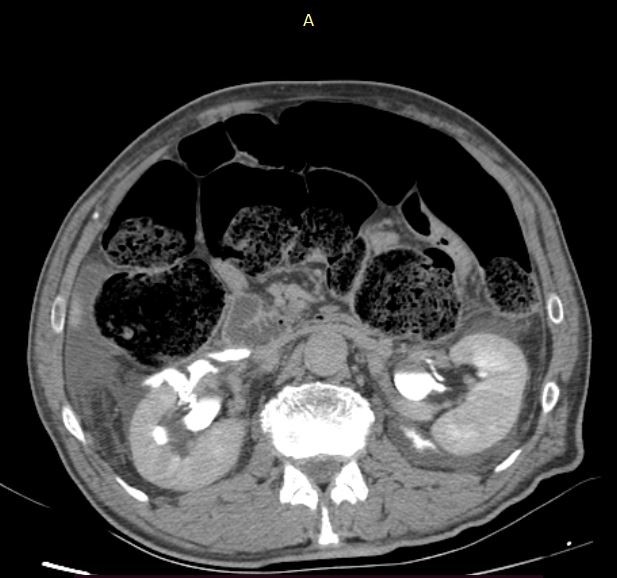
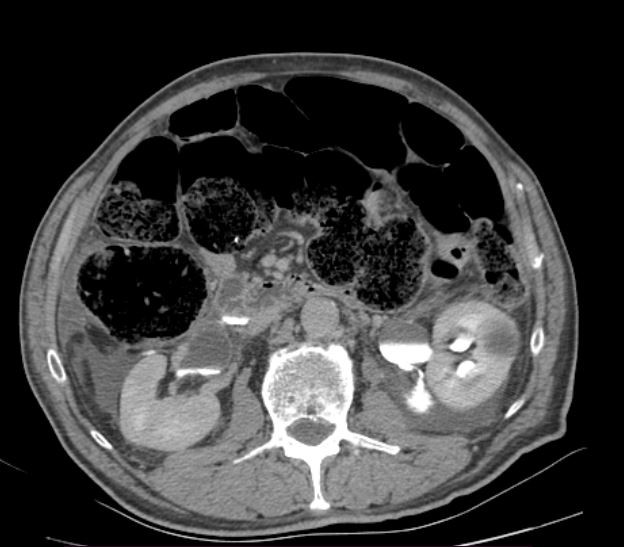
Figure 4. The exact location of the lesions of the renal pelvis and the contrast media leakage bilaterally.
Laboratory test showed increase of the C reactive proteins of 86.80mg/l which had a peak the following day, but afterwards dropped gradually. Also, there was a decrease in total protein count, as well as potassium values. There were no other significant laboratory changes which is evident from the attached table.
Table:
| Day 1 | Day 2 | Day 3 | Day 4 | Ref. Range | |
| HB/Hbg | 120.00 | 113.00 | 116.00 | 125.00 | 120.0-165.0 g/l |
| RBC | 3.92 | 3.73 | 3.82 | 4.14 | 3.8-5.8 x 109/L |
| WBC | 7.90 | 6.60 | 6.20 | 6.10 | 3.5-10.0 x 109/L |
| PLT | 243.00 | 249.00 | 299.00 | 305.00 | 150.0 -390.0 x 109/L |
| HCT | 0.35 | 0.33 | 0.33 | 0.36 | 0.35 – 0.5l/L |
| NEUT | 6.20 | 5.30 | 4.60 | 4.50 | 1.2 – 8.0 x 109/L |
| LYMPH | 1.00 | 0.90 | 0.90 | 0.90 | 1.2 – 3.2 x 109/L |
| GLUCOSE | 4.91 | 4.53 | 4.43 | 5.16 | 3.9 – 5.8 mmol/L |
| UREA | 3.80 | 5.00 | 5.40 | 3.30 | 1.8 – 9.2 mmol/L |
| CREATININE | 83.20 | 67.10 | 53.20 | 53.70 | 63.0 – 110.0 umol/L |
| CRP | 86.80 | 108.90 | 72.90 | 51.20 | 0.0 – 5.0 mg/L |
| SODIUM | 143.0 | 143.8 | 143.6 | 145.40 | 137.0-147.0 mmol/L |
| POTTASIUM | 3.06 | 3.88 | 3.21 | 4.15 | 3.6 – 5.4 mmol/L |
| TOTAL PROTEIN | 55.80 | 55.90 | 55.40 | 61.30 | 64.0 – 87.0 g/l |
| ALBUMIN | 32.50 | 33.0 | 33.90 | 35.30 | 35.0 – 52.0 g/l |
| GLOBULIN | 23.30 | 22.90 | 24.60 | 26.0 | 15.0 – 35.0 g/l |
The patient was stable and exhibited signs of recovery following the surgical placement of JJ stents in the kidneys. After 4 days the improvement was evident in the non-contrast control MDCT scans with visualization on double JJ stent in both ureters conducted after the surgical procedure. Moreover, there were no indications of any free fluid in the surrounding kidney tissue.

Figure 5. Visualization of the JJ stents and the placed urinary catheter using 3D volume rendering.
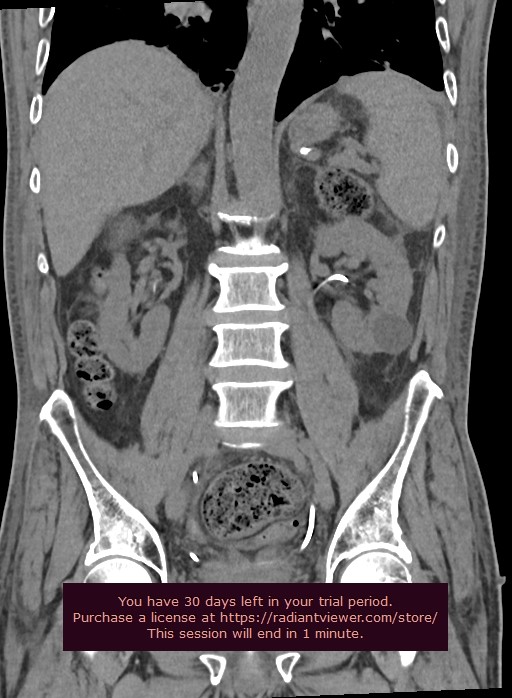
Figure 6. Control MDCT shows no trace of any free fluid in the surrounding kidney tissue after the surgical placement of the JJ stents.
Discussion
MDCT stands as the pinnacle in diagnostic imaging techniques. CT protocols typically involve scanning the abdomen and pelvis both before and after administering 100-150ml of contrast media intravenously. The critical phase for detecting a urine leak lies in the delayed phase images acquired 7-20 minutes post-injection, where the iodinated urine elevates attenuation, measured in Hounsfield Units (HU), over time, aiding in leakage visualization. Utilizing sagittal and coronal three-dimensional reformatted MDCT images, along with 3D volume rendering, proves immensely beneficial in precisely delineating the extent of the lesion. In scenarios where patients cannot receive intravenous contrast media due to allergies or have undergone renal transplantations, scintigraphy emerges as a pivotal diagnostic tool for detecting renal pelvic trauma.
Conclusion
The utilization of MDCT complemented by 3D volume rendering plays a crucial role in identifying and diagnosing renal pelvis rupture. Control examinations are necessary to confirm the successful treatment of these conditions.
References
- Cirimele V, D’amone A, Celli I et al, Isolated rupture of renal pelvis after blunt chest trauma, First description of a case, doi:10.1016/j.radcr.2023.07.032.
- Adam A, K.Dixon A, H.Gillard J et al, Grainger & Allison’s Diagnostic Radiolgoy a textbook of medical imaging, 7th edition. Elsevier Limited; 2020.p923-931.
- Catena F, DiSaverio S, Ansaloni L et al, Hot Topics in Acute Care Surgery and Trauma, CT Scan in Abdominal Emergency Surgery. Springer International Publishing; 2018.p56-62.
- Ghali AM, El Malik EM, Ibrahim AL, Ismail G, rashid M. Ureteric injuries: diagnosis, management and outcome. J trauma, 1999; 46:150-8.
- Chabukovska-Radulovska J, Spontaneous perirenal urinoma: rare complication of calculi in the ureteropelvic junction in adults; Macedonian Journal of Anaesthesia, 2019, No 7, ISSN 2545-4366, www.e-mja.finki.ukim.mk.