UDK: 616.133.3-007.64-089.844
Crcevska S.1, Janevski P.2, Stamenkovski N.2.
1PHI Health Center Skopje, Skopje
2Institute of Radiology, Faculty of Medicine, “Ss. Cyril and Methodius” University in Skopje, Republic of North Macedonia
Abstract
We present a case of a 40-years-old patient treated for brain aneurysms using a flow diverter stent for a wide-necked saccular aneurysm in the right internal carotid artery and stent-assisted embolization for a small wide-necked aneurysm in the anterior communicating artery. The intervention was executed seamlessly, showcasing a promising approach to complex aneurysm management.
Key Words:
Cerebral aneurysm; Saccular aneurysm; Flow diverter stent; Stent-assisted embolization; Endovascular techniques; Multidisciplinary approach; High-resolution imaging; Minimally invasive surgery; Internal carotid artery aneurysm; Anterior communicating artery aneurysm Preventive healthcare; Neurointervention; Advanced imaging modalities; Complex aneurysm management.
Introduction
Cerebral aneurysms are abnormal bulges in the wall of a blood vessel in the brain. Saccular aneurysms, also known as “berry aneurysms”, are the most common type, accounting for 70-80% of the cases [1, 2]. These aneurysms pose a significant risk due to the possibility of rupture, which can lead to hemorrhagic stroke and other severe neurological outcomes [3].
The management of cerebral aneurysms has evolved significantly over the years, with endovascular techniques becoming prominent due to their minimally invasive nature and favorable outcomes [4]. The traditional approach of surgical clipping, although effective, is associated with higher morbidity and longer recovery times [5]. In contrast, endovascular techniques offer a safer and more efficient alternative. Flow diverter stents and stent-assisted embolization are among the advanced techniques used to treat complex and wide-necked aneurysms. Flow diverter stents work by redirecting blood flow away from the aneurysm sac, promoting thrombosis within the aneurysm while preserving flow in the parent vessel [6, 9]. Stent-assisted embolization combines the use of a stent with coil embolization, providing structural support to prevent coil migration and ensuring effective occlusion of the aneurysm [7].
Recent advancements in imaging, such as high-resolution CT angiography and MRI, have further enhanced precision and effectiveness of endovascular interventions [8]. These imaging modalities allow for detailed visualization of aneurysm anatomy, facilitating accurate planning and execution of complex procedures. The integration of these advanced techniques has significantly improved patients’ outcomes, reducing the risk of aneurysm rupture and minimizing procedural complications [9].
This case report presents a 40-years-old male patient diagnosed with two brain aneurysms: a wide-neck aneurysm in the cavernous segment of the internal carotid artery (ACI) and a small wide-necked aneurysm in the anterior communicating artery (AcomA). What makes this case particularly interesting is the patient’s complex medical history, which posed significant challenges for treatment. The decision to employ a combined endovascular approach using a flow diverter stent and stent-assisted embolization in a single session demonstrates the versatility and efficacy of these advanced techniques in managing difficult aneurysms.
This report details the decision-making process, the procedural steps and the successful outcome, contributing valuable insights to the growing body of literature on the management of complex cerebral aneurysms.
Case Presentation
The patient is a 40-years-old male with a notable medical history of uncontrolled hypertension, borderline cholesterol and triglyceride levels and class II obesity. The patient presented with neurological symptoms characterized by retrobulbar pressure, blurred vision and diplopia. An initial ophthalmologic examination revealed extensive vascular changes, prompting further evaluation through advanced neuroimaging.
Computed tomography (CT) angiography and magnetic resonance imaging (MRI) were performed, revealing the presence of two aneurysms: a wide-necked aneurysm in the cavernous segment of the right internal carotid artery (ACI) and a small wide-necked aneurysm in the anterior communicating artery (AcomA) (Figures 1-2).
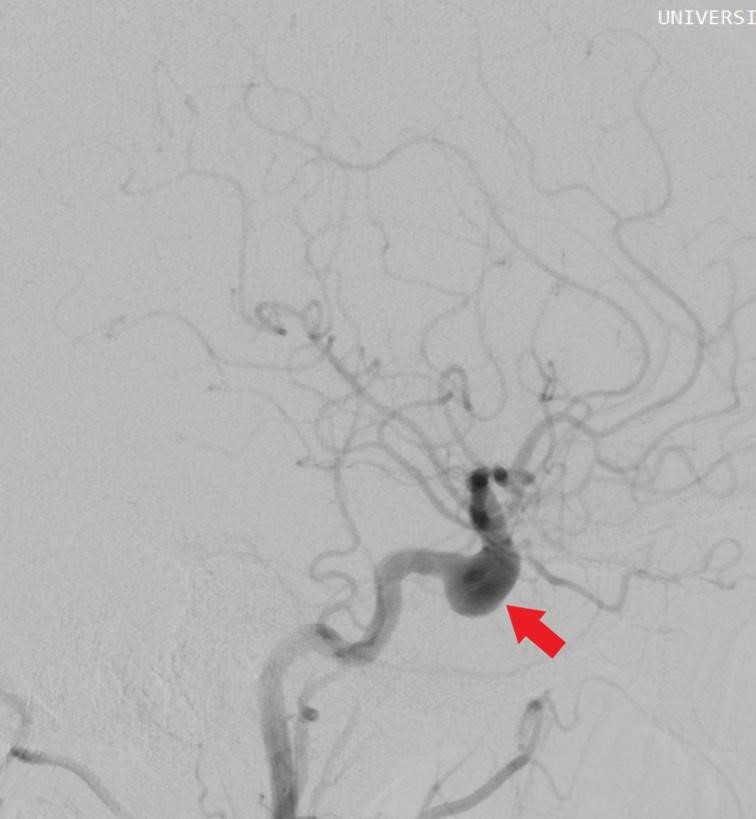
Figure 1: Saccular aneurysm in the cavernous segment of the right ACI.
Figure 2: Wide-necked saccular aneurysm in the cavernous segment of the right ACI.
Given the complexity of the aneurysms and the patient’s medical history, a multidisciplinary team decision was made to proceed with a combined endovascular approach. The procedural plan included the implantation of a flow diverter stent for the right ACI aneurysm and stent-assisted embolization for the AcomA aneurysm, executed within a single session.
Under general anesthesia, a retrograde puncture of the right common femoral artery was performed following the Seldinger technique. A long introducer sheath was advanced to the right internal carotid artery (ACI), and an access catheter was positioned. The A2 segment of the cerebral artery (ACA) was catheterized first, and a braided self-expanding stent was deployed from A2 to A1, covering the neck of the AcomA aneurysm. Immediate stasis of the aneurysm was achieved upon placement of the stent.
Subsequently, the M1 segment of the right middle cerebral artery (MCA) was catheterized, and a flow diverter stent was used to bridge the neck of the cavernous aneurysm (Figures 3). This resulted in the successful redirection of blood flow and subsequent stasis within the aneurysm sac.
Throughout the procedure, 7500 I.U. of Heparin was administered intravenously to maintain anticoagulation. Post-procedurally, the patient was transitioned to a regimen of antihypertensive medications, nonsteroidal anti-inflammatory drugs, and dual antiplatelet therapy to prevent thromboembolic complications.
Hemostasis was achieved using an AngioSeal device at the femoral artery puncture site. The intervention was completed without any immediate complications, and the patient was monitored in the intensive care unit for 24 hours post-operatively. Follow-up imaging demonstrated proper placement of the stents and successful occlusion of both aneurysms. The patient was discharged on postoperative day three, with instructions for regular follow-up and adherence to the prescribed medication regimen. At the one-month follow-up, the patient reported significant improvement in vision and no recurrence of neurological symptoms.

Figure 3. Flow divert stent in the right MCA.
Discussion
The treatment of complex cerebral aneurysms requires meticulous planning and execution, particularly when multiple aneurysms are present. In this case, the combination of a flow diverter stent and stent-assisted embolization provided a successful outcome without complications.
Flow diverter stents have revolutionized the treatment of wide-necked saccular aneurysms by redirecting blood flow away from the aneurysm sac, promoting thrombosis within the aneurysm while preserving flow in the parent vessel [6, 9, 10, 11]. This modality was effectively employed for the right internal carotid artery (ACI) aneurysm in our patient. Stent-assisted embolization, on the other hand, involves the placement of a stent across the aneurysm neck to provide a scaffold for coil embolization [4, 7]. This technique was suitable for the wide-necked aneurysm in the anterior communicating artery (AcomA), ensuring immediate stasis within the aneurysm sac [7].
This approach is backed by the latest criteria, including the 2021 updated guidelines from the American Heart Association/ American Stroke Association (AHA/ASA) for the management of patients with unruptured intracranial aneurysms [8]. These emphasize the benefits of using flow diversion and stent-assisted coiling for complex aneurysms that are not amenable to simple coiling or clipping.
When comparing this case to similar cases in the literature, our findings are consistent with studies such as those by Brinjikji et al. (2020) and Cagnazzo et al. (2018), which demonstrate the efficacy and safety of using a combination of flow diverters and stents in managing multiple aneurysms [6,7].
The decision-making process for choosing these specific interventions involved evaluating the size, shape and neck morphology of the aneurysms, along with the patient’s overall health status and risk factors such as uncontrolled hypertension and obesity. Alternative treatment options, such as microsurgical clipping or standalone coiling, were considered. However, these options were deemed less favorable due to the patient’s medical history and the anatomical challenges presented by the wide-necked aneurysms. Endovascular approaches offered a minimally invasive solution with a lower risk profile and faster recovery [12].
The outcomes of this case underscore the potential for improved patient’s prognosis through integrated treatment. The seamless execution of both interventions in a single session not only minimized the procedural risks, but also facilitated an efficient recovery process. This successful case contributes to the growing body of evidence supporting the use of advanced endovascular techniques for complex aneurysm management.
Conclusion
The successful treatment of a 40-years-old male with complex cerebral aneurysms using a combination of flow diverter stenting and stent-assisted embolization, underscores the efficacy and safety of these advanced endovascular techniques. This case highlights the importance of a multidisciplinary approach and personalized treatment plans in managing challenging aneurysms, particularly in patients with significant comorbidities.
High-resolution imaging facilitated precise diagnosis planning, leading to a seamless intervention without complications. The patient’s significant postoperative improvement underscores the advantages of minimally invasive endovascular strategies over traditional surgical methods.
This case contributes to the growing body of evidence supporting flow diverter stents and stent-assisted embolization for wide-necked and complex aneurysms. It emphasizes the necessity of preventive healthcare and adherence to medical advice in managing cerebrovascular conditions.
In conclusion, the innovative use of advanced endovascular techniques in this case exemplifies the potential for achieving excellent clinical outcomes and the evolving landscape of cerebral aneurysm management.
References
- Athre S, Albahhar M. Demystifying Interventional Radiology: A Guide for Medical Students. Springer Nature Switzerland AG; 2016, 2022.
- Marks J, Sheikh Z. Brain Aneurysms: Causes, Symptoms, and Treatment. 2023. Available from: https://www.webmd.com/brain/brain-aneurysm.
- Vogl JT, Reith, Rummeny JE. Diagnostic and Interventional Radiology. Springer-Verlag Berlin Heidelberg; 2016.
- Chalouhi N, Chitale R, Jabbour P, Starke RM, Tjoumakaris S, Dumont AS, Rosenwasser R, Gonzalez LF. Treatment of Wide-Necked Aneurysms by Stent-Assisted Coiling: The Pros and Cons. Neurosurgery. 2013; 72(2):230-238.
- Fiorella D, Woo HH, Albuquerque FC Nelson. Definitive Reconstruction of Circumferential, Fusiform Cerebral Aneurysms with the Pipeline Embolization Device. Neurosurgery. 2008; 62(5):1115-1120.
- Brinjikji W, Murad MH, Lanzino G, Cloft HJ, Kallmes DF, White PM, Kadirvel R. Safety and Efficacy of Flow Diversion for Cerebral Aneurysms: A Systematic Review and Meta-Analysis. Stroke. 2020; 51(2):520-529.
- Cagnazzo F, di Carlo DT, Cappucci M, Lefevre PH, Costalat V, Perrini P. Stent-Assisted Coiling of Intracranial Aneurysms: A Systematic Review and Meta-Analysis. AJNR Am J Neuroradiol. 2018; 39(5):838-846.
- American Heart Association/American Stroke Association. 2021 Guidelines for the Management of Patients with Unruptured Intracranial Aneurysms. 2021; 52:e282–e290.
- Lubicz B, Collignon L. Raphaeli G, Pruvo JP, Bruneau M, De Witte O, Leclerc X. Flow-Diverter Stents for the Treatment of Intracranial Aneurysms: A Prospective Study in 29 Patients. Stroke. 2010; 41():2247-2253.
- Natarajan SK, Lin N, Sonig A, Rai AT, Carpenter JS, Levy EI. The Safety of Pipeline Flow Diversion in Fusiform Vertebrobasilar Aneurysms: Multicenter Experience. Neurosurgery 2014; 75(4):455-462.
- Nelson PK, Lylyk P, Szikora I, Wetzel SG, Wanke I, Fiorella D. The Pipeline Embolization Device for the Intracranial Treatment of Aneurysms Trial (PITA): Initial Midterm Safety and Efficacy Results. Neurosurgery. 2011; 64(5):859-867.
- Pierot L, Wakhloo AK. Endovascular Treatment of Intracranial Aneurysms: Current Status. Stroke. 2013; 44(7):2046-2054.