UDK: 616-089.5:615.216.5
https://www.doi.org/10.55302/MJA2484079os
A COMPARATIVE STUDY BETWEEN DESFLURANE AND SEVOFLURANE INHALATIONAL ANESTHESIA IN ROCURONIUM CONSUMPTION DURING GENERAL ANESTHESIA WITH FENTANYL AND REMIFENTANIL
Ognjanova Simjanovska V1, Shirgoska B2, Kiprijanovska B1, Trposka A1, Naumovski F1
1University Clinic for Traumatology, Orthopedic Disease, Anesthesiology, Reanimation and Intensive Care Medicine and Emergency Department, Clinical Center “Mother Theresa”, Faculty of Medicine, “Ss. Cyril and Methodius” University, Skopje, Republic of North Macedonia
2ENT University Clinic, Medical Faculty, “Ss. Cyril and Methodius” University, Skopje
Abstract
Introduction: Rocuronium is a non-depolarizing neuromuscular blocking agent commonly used in anesthesia for muscle relaxation during surgery. It is frequently administered in combination with inhalational anesthetics like sevoflurane or desflurane, as well as opioids like fentanyl or remifentanil. They have distinct pharmacodynamic effects that can alter the required dose of rocuronium to achieve optimal muscle relaxation.
Objectives: The purpose of this study is to compare the consumption of rocuronium in four common anesthetic combinations: desflurane with remifentanil, desflurane with fentanyl, sevoflurane with remifentanil and sevoflurane with fentanyl.
Material and methods: This study included ASA I and II patients undergoing surgery who were randomly assigned into four groups. We used standard hemodynamic monitoring, the Train of Four (TOF) and the Bispectral Index System (BIS) to determine the depth of the anesthesia. We recorded the consumption of neuromuscular relaxant rocuronium in milligrams from intubation until weaking of the patient.
Results: The results obtained in both patient groups demonstrate a significantly lower consumption of rocuronium in the patients who received a desflurane inhalation anesthetic with remifentanil compared to the patients who received a sevoflurane inhalation anesthetic with fentanyl. This is thought to be due to the faster pharmacokinetic profile of desflurane, leading to an accelerated elimination in the patients, in combination with remifentanil, a short-acting opioid. Conclusion: This study contributed to an awareness of the differences in impact between the two inhalation anesthetics in the consumption of muscle relaxants for general anesthesia.
Key Words: desflurane; sevoflurane; remifentanil; fentanyl; rocuronium.
Introduction
Rocuronium is a non-depolarizing neuromuscular blocking agent (NMBA) commonly used in anesthesia for muscle relaxation during surgery. It is frequently administered in combination with inhalational anesthetics like sevoflurane or desflurane, as well as opioids like fentanyl and remifentanil. They have distinct pharmacodynamic effects that can alter the required dose of rocuronium to achieve optimal muscle relaxation. Understanding how these agents interact and influence rocuronium consumption is crucial for improving patient’s outcomes, minimizing side effects and optimizing anesthetic management (1). Rocuronium is a non-depolarizing neuromuscular blocking agent that works by competitively inhibiting acetylcholine at the nicotinic receptors on the motor endplate of skeletal muscles. This blockade prevents muscle contraction, facilitating muscle relaxation required for various surgical procedures and it is preferred for its rapid onset of action (within 1-2 minutes) and intermediate duration of effect, making it ideal for situations where quick, controlled muscle relaxation is necessary. Its effects are reversible with the administration of acetylcholinesterase inhibitors like neostigmine (2).
Desflurane and sevoflurane are volatile anesthetic agents, and they belong to the halogenated ether class and are characterized by low blood-gas solubility, which allows for rapid onset and offset of anesthesia (3). Desflurane has the lowest blood-gas partition coefficient among modern volatile anesthetics, meaning it is quickly absorbed and eliminated from the body. This characteristic makes desflurane an ideal choice for outpatient surgeries where fast recovery is desired. In terms of its impact on rocuronium, desflurane enhances the action of neuromuscular blockers, often leading to a reduced requirement for rocuronium doses. Sevoflurane is a highly volatile anesthetic that is also less irritating to the airway compared to desflurane, making it a popular choice for general anesthesia in both adults and children. Sevoflurane is associated with potent muscle relaxation and like desflurane, can reduce the need for higher doses of neuromuscular blockers. Both desflurane and sevoflurane are known to have synergistic effects with neuromuscular blockers like rocuronium. The enhancement of neuromuscular blockade, during the administration of these volatile anesthetics, allows for lower doses of rocuronium to achieve the same level of muscle relaxation. Opioid like fentanyl and remifentanil provide potent pain relief and contribute to the overall depth of anesthesia (4). These drugs work primarily by binding to μ-opioid receptors in the central nervous system, inhibiting pain transmission pathways and reducing sympathetic nervous system activity. Fentanyl is a synthetic opioid with a long duration of action compared to remifentanil. It is commonly used in combination with volatile anesthetics to provide both analgesia and anesthesia during surgery. By decreasing the sympathetic response to surgery, fentanyl can indirectly reduce muscle tone and the need for higher doses of neuromuscular blockers like rocuronium. It is particularly useful for maintaining stable hemodynamics during surgery, especially in major procedures. Remifentanil is an ultra-short-acting opioid that undergoes rapid hydrolysis by nonspecific esterase in plasma and tissues. This effect is almost immediate but short-lived, making it highly useful for procedures that require precise control over analgesia and anesthesia depth. The rapid onset and offset of remifentanil help minimize opioid accumulation and reduce the risk of prolonged muscle relaxation or respiratory depression. Remifentanil also reduces the need for higher doses of rocuronium by suppressing the autonomic nervous system.
This study will compare the consumption of rocuronium in four common anesthetic combinations: desflurane and remifentanil versus desflurane and fentanyl versus sevoflurane and remifentanil versus sevoflurane and fentanyl.
Material and Methods
This prospective, randomized, interventional clinical study was carried out at University Clinic for Traumatology, Orthopedic Disease, Anesthesiology, Reanimation and Intensive Care Medicine and Emergency Department, Skopje. We obtained approval from the Bioethics Committee of the Medical Faculty in Skopje. It took over a period of 24 months in which 120 respondents were included, 52 of whom received halogenated inhalational desflurane (MAC=0.7-1), while 68 respondents received halogenated inhalational sevoflurane (MAC=0.7-1) to administer general anesthesia. In the desflurane group, 26 subjects received fentanyl intraoperatively, while 26 subjects were maintained under anesthesia by remifentanil, and in the sevoflurane group, 34 received fentanyl, while 34 were maintained under anesthesia by remifentanil. Inclusion criteria for the study encompassed ASA 1.2 and 3 with BMI below 35 and an age limit of 18–65 years for both genders. The subjects received elective general anesthesia with an inhaled anesthetic desflurane or sevoflurane for colorectal pathology during an elective surgery lasting between 2 and 3 hours. The depth of anesthesia was monitored by the Bispectral Monitoring Index, which ranged from 45 to 55 in both groups, corresponding to stage 3 surgical anesthesia. Then the Rocuronium consumption was measured from intubation until weaking of the patient. The study’s exclusion criteria were ASA over 3, age under 18 and over 65 years, morbid obesity, BMI over 35, existence of neuromuscular diseases, history of possible malignant hyperthermia, obstructive lung disease with regular use of bronchodilators and the presence of preoperative cognitive disorder, which originates from chronic opioid or benzodiazepine use, as well as cerebrovascular disorders.
In the operating room, patients were connected to a monitor to observe the ECG, non-invasive blood pressure, pulse oximetry, and Bispectral Index. A peripheral neurostimulator was installed to monitor The Train of Four (TOF). Patients were reoxygenated with 100% oxygen within 3 minutes with a flow of fresh gases of 6L/min and anesthesia was induced with a standardized induction approach using sedative midazolam 0.03mg/kg iv., fentanyl 1-2mcg/kg, propofol 2mg/kg and muscle relaxant rocuronium 0.6mg/kg. The respiratory pathway is secured with an adequately-sized endotracheal tube and connected to an anesthesiology ventilation machine with an inhaled anesthetic desflurane (3–6%), (1–2%) to MAC=0.7–1, with a flow of fresh gases of 2L/min, 50% air with 50% oxygen. Tidal capnography etCO2, the inspiratory faction (Fi) of anesthetic gases and the expiratory faction (FE) of volatile anesthetics are monitored. Minute ventilation is set with a respiratory volume of 6–8ml/kg, a 12/min respiratory frequency and an inhale exhale ratio of 1:2 to maintain a 30–40mmHg CO2 tidal. The dosage for maintenance of intravenous and inhaled anesthetic agents is titrated to maintain BIS from 45–55. Additional bolus doses of fentanyl at a dose of 0.5mcg/kg were given as needed. Remifentanil was given at a dose of 0.125–0.25mcg/kg/min. Muscle relaxation was maintained with intermittent doses of rocuronium at a dose of 0.15mg/kg. The volatile anesthetic was reduced 15 minutes before the surgery ended to MAC=0.5 and was interrupted after the last surgical stitch was placed. The flow of fresh gases was then increased to 6L/min with 100% oxygen. After achieving TOF ≥ 3, a reversion of the neuromuscular block with Neostigmine 0.03mg/kg and Atropine 0.01mg/kg was administered iv.
Results
The statistical analyses were performed using SPSS version 26. The significance threshold, for
all statistical analyses, was set at p<0.05. To compare the data, a student’s T test was employed. The sample size was 120 subjects. Both groups were comparable in demographic data. The patients were aged from 55.2 to 65 years, and the average age was 62±2.5 years. The gender structure of the patients consisted of 54 (45%) women and 66 (55%) men. According to the ASA value, 54 (45%) patients had score 3, 52 (43.33%) had score 2 and 14 (11.67%) had ASA 1. The body mass index ranged from 20.1 to 28.2kg/m2, on average was 23.8 ± 1.9kg/m2.
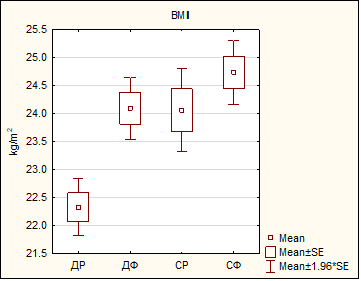
For p=0.000001, an overall statistically significant difference between the analyzed groups was confirmed in terms of Body Mass Index, which, with post-hoc analysis, was shown to be due to a significantly lower BMI in the desflurane remifentanil group versus the desflurane fentanyl group (22.33±1.4 vs 24.09±1.5kg/m2, p=0.0006), versus the sevoflurane remifentanil group (22.33±1.4 vs 24.06±2.1kg/m2, p=0.00075), and, versus the sevoflurane fentanyl group (22.33±1.4 vs 24.73±1.6kg/m2, p=0.00014) (Table 1, 1a, Figure 1).
Table 1. BMI of patients in the desflurane remifentanil, desflurane fentanyl, sevoflurane remifentanil and sevoflurane fentanyl groups.
| Statistical parameters | Group | |||
| Desflurane
Remifentanil |
Desflurane
Fentanyl |
Sevoflurane
Remifentanil |
Sevoflurane
Fentanyl |
|
| BMI (kg/m2) | ||||
| mean ± SD | 22.33±1.4 | 24.09±1.5 | 24.06±2.1 | 24.73±1.6 |
| min- max | 20.1 – 25.1 | 21.8 – 27.1 | 21.1 – 28.2 | 21.3 – 27.1 |
F (Analysis of Variance)
Table 1a. Tested intergroup differences in patients’ BMI
| F=11.31 ***p=0.000001; Tukey HSD test | |||
| Group | Desflurane
Fentanyl |
Sevoflurane
Remifentanil |
Sevoflurane
Fentanyl |
| Desflurane Remifentanil | ***p=0.0006 | ***p=0.00075 | ***p=0.00014 |
| Desflurane Fentanyl | p=1.0 | p=10.45 | |
| Sevoflurane Remifentanil | p=10.42 | ||
F (Analysis of Variance); post-hoc Tukey honest test.
***sig p<0.0001
| DR DF SR SF |
| Figure 1. Mean BMI in the desflurane remifentanil, desflurane fentanyl, sevoflurane remifentanil, and sevoflurane fentanyl groups.
|
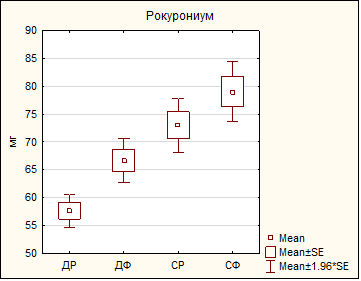
An overall statistically significant difference was confirmed in terms of the Rocuronium value (p<0.0001), which with post-hoc analysis, was shown to be due to significantly lower consumption of muscle relaxant given intraoperatively in the desflurane remifentanil group compared to the three other groups: desflurane fentanyl group (57.67±8.2 vs 66.67±10.9mg, p=0.025), sevoflurane remifentanil group (57.67±8.2 vs 73.0±13.4mg, p=0.000152) and sevoflurane fentanyl group (57.67±8.2 vs 79.0±14.9mg, p=0.000137), as well as significantly lower consumption in the desflurane fentanyl group compared to the sevoflurane fentanyl group. (66.67±10.9 vs 79.0±14.9mg, p=0.00092) (Table 2, 2a, picture 2).
Table 2. Consumption of rocuronium in desflurane remifentanil, desflurane fentanyl, sevoflurane remifentanil and sevoflurane fentanyl groups.
| Statistical parameters | Group | |||
| Desflurane
Remifentanil |
Desflurane
Fentanyl |
Sevoflurane
Remifentanil |
Sevoflurane
Fentanyl |
|
| Rocuronium/mg | ||||
| Mean ± SD | 57.67±8.2 | 66.67±10.9 | 73.0±13.4 | 79.0±14.9 |
| Min – max | 50 – 70 | 50 – 90 | 50 – 90 | 50 – 100 |
Table 2a. Tested between-group differences in consumption of rocuronium.
| F=16.95 p=0.000000 Tukey HSD test | |||
| Group | Desflurane
Fentanyl |
Sevoflurane
Remifentanil |
Sevoflurane
Fentanyl |
| Desflurane Remifentanil | *p=0.025 | ***p=0.000152 | ***p=0.000137 |
| Desflurane Fentanyl | p=0.19 | ***p=0.00092 | |
| Sevoflurane Remifentanil | p=0.23 | ||
F (Analysis of Variance); post-hoc Tukey honest test.
*sig p<0.05, ***sig p<0.0001.
| DR DF SR SF |
| Figure 2. Mean consumption of rocuronium in the desflurane remifentanil, desflurane fentanyl, sevoflurane remifentanil and sevoflurane fentanyl groups.
|
Discussion
The consumption of rocuronium is influenced by various factors including the type and dose of anesthetics administered. Desflurane potentiates the effects of neuromuscular blocking agents like rocuronium and the exact mechanisms underlying this potentiation are not fully understood but is believed to involve interactions at both the spinal cord and neuromuscular junction. The use of remifentanil with its rapid onset and offset can provide a high degree of intraoperative control over anesthesia depth further reducing the need for larger doses of rocuronium. Rapid metabolism ensures that it does not accumulate and minimize prolonged muscle relaxation or respiratory depression following surgery. A comparable outcome was reported in the study of Maidatsi et al., that desflurane anesthesia significantly prolongs the duration of action of rocuronium at 0.9mg/kg −1 single bolus dose, compared to sevoflurane or propofol anesthesia maintenance regimens (5). Our findings suggest that the group desflurane remifentanil had significantly lower consumption of muscle relaxant given intraoperatively compared to the three other groups. Significant difference was shown to be due to lower consumption of rocuronium given intraoperatively in the desflurane remifentanil group 57.67±8.2mg compared to the sevoflurane fentanyl group 79.0±14.9mg. Same results were presented in the study of Moriyama et al., that neuromuscular relaxation effects were found to be stronger when using inhaled anesthesia, especially desflurane (6). Both desflurane-remifentanil and sevoflurane-fentanyl provide excellent hemodynamic stability during surgeries, but remifentanil, when used with desflurane, tends to offer slightly more precise control over hemodynamic fluctuations, especially in high-stress surgeries. This enables an overall decrease in the required doses of rocuronium, as muscle tone and autonomic responses are more finely tuned. Regarding their adjustment in dosage, ensured optimal muscle relaxation is attained, with a minimum of drug-related side effects such as postoperative residual neuromuscular blockade.
Conclusion
The resulting values obtained from this study showed a statistically significant difference. Desflurane combined with remifentanil has a lower consumption of rocuronium due to the synergistic effects of desflurane on neuromuscular blockade and the rapid metabolism of remifentanil. As showed in the results, sevoflurane combined with fentanyl results in a significantly higher dose of rocuronium. Intraoperative rocuronium consumption is influenced by the choice of anesthetic agents like the inhalational anesthetics and opioids used. This study contributed to an awareness of the differences in impact between the two inhalation anesthetics in the consumption of muscle relaxants for general anesthesia in clinical practice. Understanding the interactions between these anesthetics is essential for optimizing anesthesia management, minimizing drug-related side effects and ensuring safe and effective surgical outcomes. Further research into these interactions will continue to improve clinical protocols and enhance patients’ outcomes.
References:
- Radkowski P, Krupiniewicz KJ, Suchcicki M, Machoń NJ, Cappello S, Szewczyk M, Wolska JM, Stompór T. Navigating Anesthesia: Muscle Relaxants and Reversal Agents in Patients with Renal Impairment. Med Sci Monit. 2024 Aug 27;30:e945141. doi: 10.12659/MSM.945141. PMID: 39188037; PMCID: PMC11365435.
- Kim YB, Sung TY, Yang HS. Factors that affect the onset of action of non-depolarizing neuromuscular blocking agents. Korean J Anesthesiol. 2017 Oct;70(5):500-510. doi: 10.4097/kjae.2017.70.5.500. Epub 2017 Sep 28. Erratum in: Korean J Anesthesiol. 2017 Dec;70(6):656. doi: 10.4097/kjae.2017.70.6.656. PMID: 29046769; PMCID: PMC5645582.
- Khan J, Patel P, Liu M. Desflurane. [Updated 2024 Feb 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537106/.
- Lee S, Ro YJ, Koh WU, Nishiyama T, Yang HS. The neuromuscular effects of rocuronium under sevoflurane-remifentanil or propofol-remifentanil anesthesia: a randomized clinical comparative study in an Asian population. BMC Anesthesiol. 2016 Aug 22;16(1):65. doi: 10.1186/s12871-016-0231-0. PMID: 27549387; PMCID: PMC4994310.
- Maidatsi PG, Zaralidou ATh, Gorgias NK, Amaniti EN, Karakoulas KA, Giala MM. Rocuronium duration of action under sevoflurane, desflurane or propofol anaesthesia. European Journal of Anaesthesiology. 2004;21(10):781-786. doi:10.1017/S0265021504000055.
- Moriyama, T., Irie, Y., Mukaihara, K. , Ishizuka, K. , Matsunaga, A. and Kanmura, Y. (2016)Continuous Rocuronium Administration Method Based on Pharmacokinetic/Pharmacodynamics Model during Propofol, Sevoflurane, and Desflurane Anesthesia. Open Journal of Anesthesiology, 6, 77-84. doi:4236/ojanes.2016.65013.