UDK: 616.056.7:618.5-089.888.61
SUCCESSFULLY COMPLETED PREGNANCY IN A PATIENT WITH KLIPPEL FEIL SYNDROME (KFS)
Irena Todorovska, Igor Samardziski, Slagjana Simeonova Krstevska, Dabeski D., Livrinova V.
University Clinic of Gynecology and Obstetrics, Skopje
КFS is a congenital anomaly characterized by fusion of two or more cervical vertebrae. The main three manifestations are a low hairline, a short neck and limited neck movement. This syndrome can cause chronic headache and neck and back pain (1).
It was described by Maurice Klippel and Andre Feil separately. The exact incidence of this disorder is unknown. It is assumed to be around 42,000-50,000 livebirths. It occurs more often in female individuals (about 65%). КFS type 2 is the most common one(2).

In КFS, it may be accompanied by other conditions and abnormalities:
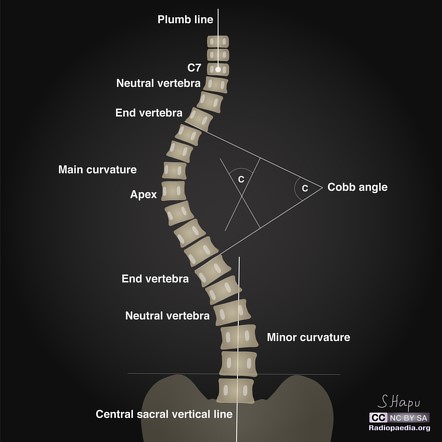
– Scoliosis,
– Cervical dystonia,
– Genitourinary abnormalities,
– Sprengel deformity (small and not lowered scapula),
– Heart deformities,
– Pulmonary abnormalities and respiratory problems,
– Hearing problems,
– Facial asymmetry,
– Torticollis,
– Central nervous system abnormalities,
– Other skeletal abnormalities,
– Situs inversus,
– Synkinesis (movements of one hand involuntarily imitate the intentional movement of the other hand).
The exact cause and mechanism of КFS is not exactly known. Medical research believes that КFS occurs when embryonic tissue that normally develops into individual vertebrae does not divide correctly (3).
Isolated КFS may be sporadic or hereditary. КFS can sometimes occur as a combination of genetic and environmental factors, mutations, and at least 3 genes are associated with the onset of КFS.
Sometimes, КFS occurs randomly, and sometimes it is genetic and runs in several family members. Autosomal dominant and autosomal recessive inheritance, with different genes (4).
When КFS is caused by mutations in GDF6 or GDF3, it is inherited in an autosomal dominant manner.
When КFS is caused by mutations in the MEOX1 gene, it is inherited in an autosomal recessive manner (4,5).
КFS is diagnosed by clinical evaluation, identification of characteristic physical findings and specialized tests. Diagnosis begins with X-rays or other advanced imaging techniques, such as Magnetic Resonance, which shows fusion of the cervical vertebrae, open spaces (interspaces) between the vertebrae and possible pressure on the spinal cord. X-rays of the entire spine are performed to detect other spinal abnormalities. КFS can be associated with a wide range of abnormalities involving other parts of the body. Therefore, it is necessary to do:
– Examination of the chest to determine the disorder of the heart and lungs.
– Examination of the chest to detect abnormalities of the ribs.
– MRI for spinal stenosis or neurological deficit.
– Ultrasound of the kidneys or renal anomalies.
– Hearing evaluation due to high incidence of hearing loss.
– Various laboratory tests to determine the functioning of the organs (5).
Treatment: There is no cure for this syndrome. Therapy is symptomatic and supportive. Careful evaluation, continuous follow-up, and coordination of multiple specialists are required to improve outcome, and additional scans may be needed to determine the exact abnormality (6).
Neck collar, traction, physical therapy, non-steroidal anti-inflammatory drugs, analgesics can be used. In most people, the symptoms are progressive due to the degenerative changes that occur in the spine.
Surgical intervention may be indicated for various reasons, such as persistent pain, neurological deficit, neck instability, spinal cord constriction or to correct severe scoliosis. Sometimes surgical intervention is needed to improve other skeletal anomalies, or those associated with the heart, kidneys, etc.
Those with an increased risk of neurological complications should be regularly monitored by health professionals and advised to avoid activities that may lead to trauma or injury to the cervical vertebrae.
The prognosis for people with CFS varies depending on the specific characteristics and severity of the affected person. People with minimal fusion of the cervical vertebrae can lead a normal, active life and may not have significant restrictions. People with severe forms of CFS require close monitoring but may have a good prognosis if symptoms and complications are properly treated (7).
Case Report
Our patient is thirty years old, with a fixed diagnosis of Klippel-Feil syndrome, thoracis scoliosis, pre-existential hypertension, deafness. At the age of one year, cheilognathopalatoschisis was corrected, nephrolithiasis was present.
At the University Clinic of Gynecology and Obstetrics, the patient appears for the first time at 24.3 weeks of gestation, in an outpatient clinic where she has a scheduled screening examination in the second trimester.
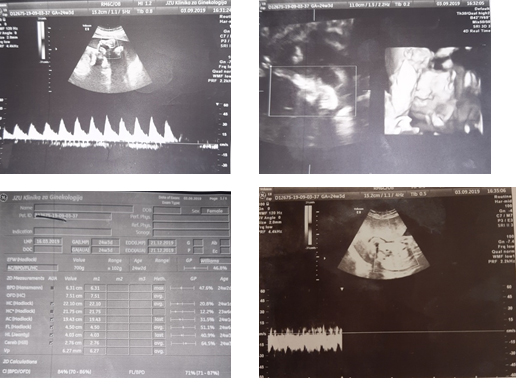
During the examination, it was established that it was a eutrophic fetus, without major anomalies, normal fetoplacental flow, normal fetal movements. A recommendation was given to do control examinations at the Clinic for Pulmonology, Orthopedics, Cardiology and Nephrology. At the control examination after 1 week, the patient had an examination only at the Pulmonology and Orthopedics Clinic, where appropriate therapy was prescribed. Laboratory analyzes were in reference values. Blood pressure was regulated by antihypertensive therapy.
The next two controls were on a weekly basis until the 27th gestational week, when, due to malignant hypertension, she was initially admitted to the Department of Pathological Pregnancy, and then transferred to the Department of Peripartum Intensive Care. During the hospitalization, therapy for fetal lung maturation, antihypertensive and neuroprotective therapy was prescribed. A series of council examinations were performed by a nephrologist, cardiologist (correct findings), pulmonologist and otorhinolaryngologist. It was communicated with the patient with a sign language professional.
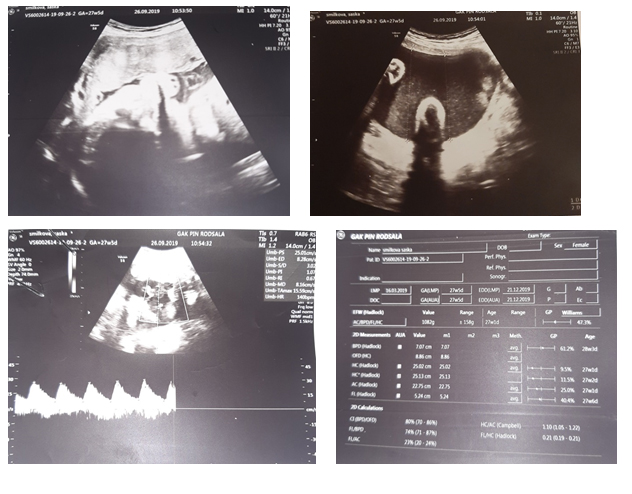
During hospitalization, high values of the angiogenic factors sFLT/PLGF up to 793.05, proteinuria 0.79g/L and malignant hypertension regulated by double antihypertensive therapy were determined. NST was reactive. The ultrasound finding was normal, the fetus had a normal fetoplacental flow.
After detailed anesthetic preparation, the patient was delivered by elective caesarean section at 28.5 weeks of gestation and a live female fetus was obtained with RTM=920g/35cm and AS=6/7/7. The intervention went smoothly. Postoperatively, the hypertension was regulated, the wound healed per primam, and she was discharged from the clinic on the third postoperative day. After 82 days of stay in the Department of Intensive Care and Therapy, the newborn was discharged in a stable condition and current weight of 1920g.
A few years later, it can be seen that the newborn is developing normally. I am happy that the girl has normal growth and development and does not lag behind her peers. A mother is filled with love and has a purpose in life. A beautiful picture of a happy family.
Although the syndrome is rare and described disorders make treatment difficult, with careful preparation, the pregnancy can be successfully terminated. Difficulties can be successfully overcome with a multidisciplinary approach.
REFERENCES
1) Driscoll DJ, Rigamonti D, Gailloud P. Klippel-Feil Syndrome. NORD Guide to Rare Disorders. Lippincott Williams & Wilkins. Philadelphia, PA. 2003:720.
2) Tassabehj M, Fang ZM, Hilton EN, et al. Mutations in GDF6 are associated with vertebral segmentation defects in Klippel-Feil syndrome. Hum Mutat. 2008; 29:1017-1027.
3) Paul I, Badmanaban B, Campalani G. Patients with Klippel-Feil syndrome should have imaging of the subclavian artery and its branches prior to coronary artery bypass grafting. Interact Cardiovasc Thorac Surg. 2007; 6:403-405.
4) Vaidyanathan S, Huges PL, Soni BM, Singh G, Sett P. Klippel-Feil syndrome – the risk of cervical spinal cord injury: a case report. BMC Family Practice. 2002; 3:6.
5) Clarke RA, et al. Heterogeneity in Klippel-Feil syndrome: a new classification. Pediatr Radiol. 1998; 28:967-74.
6) McGaughran JM, et al. Audiological abnormalities in the Klippel-Feil syndrome. Arch Dis Child. 1998; 79:352-55.
7) Rouvreau P, et al. Assessment and neurologic involvement of patients with cervical spine congenital synostosis as in Klippel-Feil syndrome: study of 19 cases. J Pediatr Orthop B. 1998; 7:179-85.