14. UDK: 616-006.6-055.1
Petrovska T1,2, Cabukovska Radulovska J1,2, Sofrnjevska Glavinov M1,2, Danailova M2
1 PHI University Clinic of Surgery “St. Naum Ohridski” – Skopje
2Faculty of Medical Sciences, University “Goce Delchev”, Shtip
Abstract
Breast cancer in men is very rare with an incidence of 1 in 800 (1), but it can occur in the presence of gynecomastia and presents as intraductal carcinoma. Lobular carcinoma does not occur because these lobules are not developed in men. We present a case of a 69-years-old patient who, 1 month before examination, palpated a small lump in the right breast. Ultrasound, mammography and core biopsy of the lesion were performed, and intraductal invasive carcinoma of the breast was diagnosed.
Key Words: core biopsy, intraductal carcinoma, mammography, men, ultrasound,
Introduction
Physiology of the Breast Embryology: The rudimentary and totipotent glands of the breasts in males and females are identical at birth, composed of mammary lobules that are drained through milk ducts to the nipple. In boys during prepubertal period, testosterone levels increase leading to atrophy of the mammary parenchyma. Whereas in girls during the peri-pubertal period, there is an increase in estrogen levels which results in accelerated branching and proliferation of the milk ducts, while progesterone stimulates the formation of terminal ductal-lobular units (TDLU). If boys experience transient elevation of serum estradiol levels, there will be proliferation of subareolar ducts and stroma. This condition normalizes when testosterone levels begin to rise and reach adult normal values.
Normal Male Breast consists of skin, subcutaneous adipose tissue and atrophic ducts. Cooper’s ligaments are absent. The development of lobules, which are provoked by estrogen and progesterone, is exceptionally rare. (Rarely, fibroadenomas, phyllodes tumors, invasive lobular carcinoma, as well as lobular carcinoma in situ develop.) (2).
Conditions associated with proliferation of stroma and milk ducts can occur in men, such as gynecomastia, invasive ductal carcinoma and ductal carcinoma in situ. The male breast is susceptible to the same pathological processes as the female breast. Large number of conditions are differentiated using mammography, ultrasound and even breast MRI. The initial modalities are mammography and ultrasound, and if there is suspicion of malignancy, breast biopsy is performed.
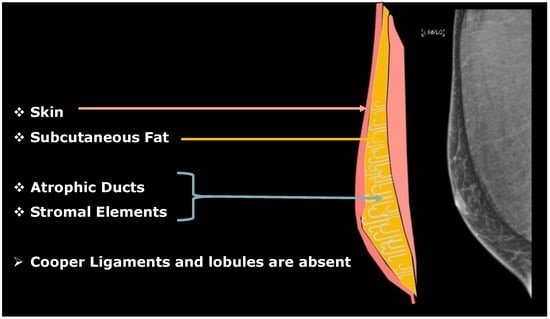
Figure 1. Anatomy Illustration of the Male Breast.
Breast cancer in men is extremely rare, representing about 0.25% of malignancies in men and 0.5%-1% (2) of all breast cancers (in both genders). The incidence of male breast cancer in the USA has increased from 0.85 to 1.3 per 100,000 men in the period from 1972 to 2000. The ratio of female to male cases is 100:1 in whites and 70:1 in blacks (4). Diagnosis of this type of cancer is often delayed due to men’s lack of awareness and information about this condition to seek advice. The definitive diagnosis is made through histopathological examination, typically obtained via core biopsy. Benign breast neoplasms in men include angiolipoma, schwannoma, intraductal papilloma and lipoma. Additionally, conditions such as lymphadenitis, sebaceous cyst, diabetic mastopathy, fat necrosis, subareolar abscess, breast enlargement, venous malformations, hematoma, etc., can occur. Sometimes, these conditions may have similar radiological expression, but with the use of all radiological methods, a diagnosis can be reached. The definitive histopathological diagnosis is obtained after core biopsy.
Materials and Methods
We present a case of a 69-years-old patient with a lump behind the right nipple in the superolateral quadrant, which he noticed one month before. He was at that moment receiving therapy for prostate issues – Tamsulosin (brand name: Tamsulosin) Prostatitis Max Forte (has been taking it for the last 5-6 years). Two years ago, he underwent surgery to remove a left testicular Leydig cell tumor.
On inspection, a lump in the right breast was noted. Palpation reveals a hard consistency.
Mammography findings: Bilaterally, there are features suggestive of female-type breast parenchyma retroareolar. An oval shadow is demarcated towards 11 o’clock in the right breast. The left breast shows no focal densities. There are no pathological calcifications. Axillary lymph nodes are visible in both axillae.
BI-RADS 3. Core biopsy of the lesion is recommended.


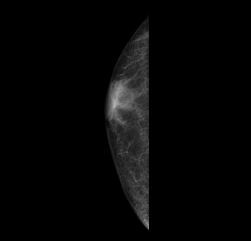
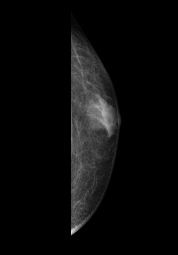
Figure 2. Mammography MLO and CC Projection – Gynecomastia with a small oval density on the baseline mammogram in the superolateral quadrant of the right breast.
Ultrasound findings: Bilateral axillary lymph nodes with normal morphology are observed. Bilaterally, there is poorly developed breast parenchyma retroareolar. On the right, at 0.5cm from the nipple towards 10 o’clock, a hypoechoic hypo-vascular change with dimensions of 0.76 x 0.45cm and EI 2.70 is visualized. The left breast shows no demarcated pathological echogenicity. BI-RADS 0. Recommendation: Biopsy of the change in the right breast is advised.

Figure 3. Ultrasound of the lesion in the right breast – Hypoechoic oval clearly demarcated lesion.

Figure 4. Elastography of the lesion showing a strain ratio of 2.70.
Core biopsy of the lesion in the right breast, measuring 0.45cm, was performed under aseptic conditions using a 14G needle, and 2 samples were taken for histopathological analysis.
Histopathological findings: Microscopically, the delivered material consists of fragments of male breast tissue, partly infiltrated by neoplastic tissue composed of atypical cells with moderate nuclear grade, arranged in solid nests. Additionally, the immunohistochemical analysis yielded the following results: mammaglobin (-), podoplanin (-), GATA3 (+), SMA (-). The findings are consistent with invasive breast carcinoma, NG2.
Discussion
Breast cancer in men, although rare, can lead to fatal outcomes. This condition may sometimes occur alongside gynecomastia. If there is a subareolar eccentrically positioned lump, it should be followed up with mammography and breast ultrasound. If there is suspicion of malignancy, biopsy should be performed. Conditions associated with proliferation of stroma and milk ducts, such as gynecomastia, invasive ductal carcinoma, and ductal carcinoma in situ, can occur in men. Patients with genetic mutations BRCA1-2 should undergo annual mammography screening.
Conclusion
Breast cancer in the male population does exist, albeit rare, but it should be considered when there is a lump in the breasts. There is a need to raise awareness among men about this condition, especially if there are additional factors such as gynecomastia or genetic mutations.
Increasing awareness among the male population about the existence of breast cancer can reduce morbidity and mortality from this disease through timely radiological evaluation.
References
- KoppanBreast Imaging (Kopans, Breast Imaging) Third Edition.
- Omene C, Tiersten A (2010) The differences between male and female breast cancer. In: Legato MJ (Ed) Principles of gender-specific medicine. Elsevier, pp 459–472. https://doi.org/10.1016/b978-0-12-374271-1.00042-3.
- Nguyen C, Kettler MD, Swirsky ME et al. Male breast disease: pictorial review with radiologic-pathologic correlation. Radiographics. 2013; 33(3):763–779. https://doi.org/10.1148/rg.333125137.
- Cheri Nguyen, Mark D. Kettler, Michael E. Swirsky, Vivian I. Miller, Caleb Scott, Rhett Krause, and Jennifer A. HadroMale Breast Disease: Pictorial Review with Radiologic-Pathologic Correlation RadioGraphics 2013 33:3, 763-779.
- Giordano SH. Breast cancer in men. N Engl J Med 2018; 378(24):2311–2320.
- American Cancer Society. Key statistics for breast cancer in men. Available at: https://www.cancer.org/cancer/breast-cancerin-men/about/key-statistics.html. Accessed October 16, 2022.
- Jeong Geun Yi, M.D., Kyung Joo Park,et al. Radiologic Findings of Male Breast Cancer: A Case Report. Journal of the Korean Radiological Society, 1994: 31 (4): 759-761.
- D’Angelo, A, Portaluri, A, Caprini, F. et al. Male Breast: A Review of the Literature and Current State of the Art of Diagnostic Imaging Work-Up. Diagnostics 2023, 13, 3620. https://doi.org/10.3390/diagnostics13243620.
- American Cancer Society. Breast cancer facts and figures 2022–2024. Available at: https://www.cancer.org/research/ cancer-facts-statistics/breast-cancer-facts-figures.html. Accessed October 16, 2022.